

The Cognitive Prosthetic
How large language models change clinical judgment, responsibility, and training
I’ve been watching myself and how I work. My workflow in the clinic has totally changed. I’ve felt it and my clinic nurses have noticed it. I hid my use initially, but not now.
It’s medical LLMs, and they’ve revolutionized my relationship to information. I’ve moved from recalling medical knowledge to retrieving and applying it in real time at the point of care.
For simplicity, I’ll refer to tools like OpenEvidence and DoxGPT as mdGPTs, i.e., medical LLMs built for clinicians. Some physicians still use ChatGPT for medical questions. I’d recommend using purpose-built medical tools.
For the uninitiated, these are large language models designed to help doctors quickly access the answers to questions. From drug dosing to current treatment guidelines, mdGPTs scour the medical information domain for answers to just about any question a doctor could have. If you’ve used ChatGPT for your personal use, this is similar but built for a medical audience. I initially wrote about this over the summer here. At the time these tools were new to me.
I sometimes call these cognitive prosthetics. So if you see that term in future letters, you’ll know what I’m talking about.
Like most changes I discuss here, we don’t see them coming. They kind of creep in. Doctors are clearly using these tools, although I think it continues to be a minority of the working population around me based on my own observations.
A short history of my relationship to information
I know folks don’t care about where we’ve come from, but I think a little historical context might show how different things became only recently.
Here’s how I got information over my career (And I’ll make this quick):
Early career — Honestly, I rode on what I had been taught in residency and fellowship. Beyond that, my information came from paper journals. This usually meant going to the library to pull journals. Super high friction. It required big motivation to get the answer.
Mid career — Journals arrive on the internet. While the barrier to access was lower, I still had to find the best article, grab the PDF, and then read and process it. So, lower friction than going to the library, but still not easy when I had a quick question. It’s super rare that I accessed journal articles on my phone, again due to the effort. UptoDate landed as a web-based, searchable product in 2001. This lowered friction further and brought us from getting information to finding answers.
Now — Since 2023 mdGPTs have been available to most physicians with a smartphone. My questions are answered with references in a matter of several seconds. It’s crazy. It’s not just faster, it’s conversational synthesis at the point of care: you can find the answer, iterate, and get context plus citations in real time.
MDGPT in front of patients
I have bridged over to using these tools with patients. Case in point:
Last week in clinic I was seeing a new consult on a school-aged child with severe reflux who had been begun on a PPI prior to seeing me. He was dramatically better and was seeing me for a long-term plan. There was a history of Helicobacter pylori in the family and we discussed urea breath testing and stool antigen tests. But being on a PPI we couldn’t do it. The family asked about a blood test. We don’t use that but I had forgotten the specifics around the limitations of serology.
I had my answer in a few seconds and shared it with the family.
I don’t think that the family thought less of me for not having that at my fingertips. In fact, I think they were impressed in the way I conjured an answer that perfectly fit our dilemma. Most importantly, I offered context that helped shape a plan that everybody was happy with.
In pediatrics we often face patients with rare genetic syndromes. And every pediatric health professional knows we can’t keep our fingers on all of these. Early in my career I referenced Smith’s Recognizable Patterns of Human Malformation, mid-career I’d Google the syndrome and hope there was a summary publication linked on first page, and now there’s mdGPT.
And it changes everything.
What does this indicate?
For physicians, this marks the ultimate movement from knowing things and working with what’s in our head to instantly accessing information and knowledge. Again, we had access to the internet before, but the friction was too high for minute-to-minute utility.
Now I find myself looking for answers to questions that I knew the answer to but didn’t know why. Given the stage of my career, it’s an interesting tool for exploring things that I’ve noticed but not been fully able to articulate.
And if you think you’ve got this stuff all in your head after years of practice, you probably haven’t kicked the tires on these things.
This is the crazy question: do we really need to know anything? It’s navel gazing but it forces the deeper issue of what we access versus what we need to know.
We went through some of these exercises when the internet was rising. Memorization of the Krebs cycle was the first topic of debate. If we can look it up with the tool in our pocket, why would we need to memorize it? And then came the question, who actually references the Krebs cycle?
Where could this go?
A few loaded thoughts about where instant access to information and knowledge could land. I’ll build these out more completely in coming letters, but some teasers to get you thinking:
1. Competence is redefined
For most of my career, competence began with what I could carry around in my head but heavily influenced by judgment. The internet loosened that, but mdGPTs have leveled it. The hard part isn’t ‘answers’, it’s the responsibility and weighing tradeoffs. I become a high-level interpreter, or docent.
When information is cheap, judgment becomes the scarce thing. Our role will migrate to stewardship around easily accessible knowledge.
Maybe it’s my new job?
2. The creation of two layers of medicine
I can see a commoditized baseline medicine that’s contrasted with a kind of high-bandwidth medicine. Baseline care would be protocol-like care (by patient, APP, or urgent care professional, with tool support). High bandwidth care would be context-heavy care (values, nuance, uncertainty).
I could even imagine more than two layers of medical care.
3. A shift in the standard of care
Here’s a wild thought: Once answers are ambient, the system will come to expect them. When everyone has access to the same thinking tools, who gets punished for not walking in lock-step? What if you don’t check your work?
4. Total reconfiguration of medical training
Look at all of these potential changes and then ask yourself: How do you prepare the next generation of doctors for this? We’ll either train judgment or we’ll mint commodity clinicians who can’t tell when the screen is FOS.
Pro-tip: Watch the workflows. That’s where all this stuff shows up first.
If you’re using OpenEvidence or DoxGPT in your own clinic, I’d like to hear how they’re changing you.
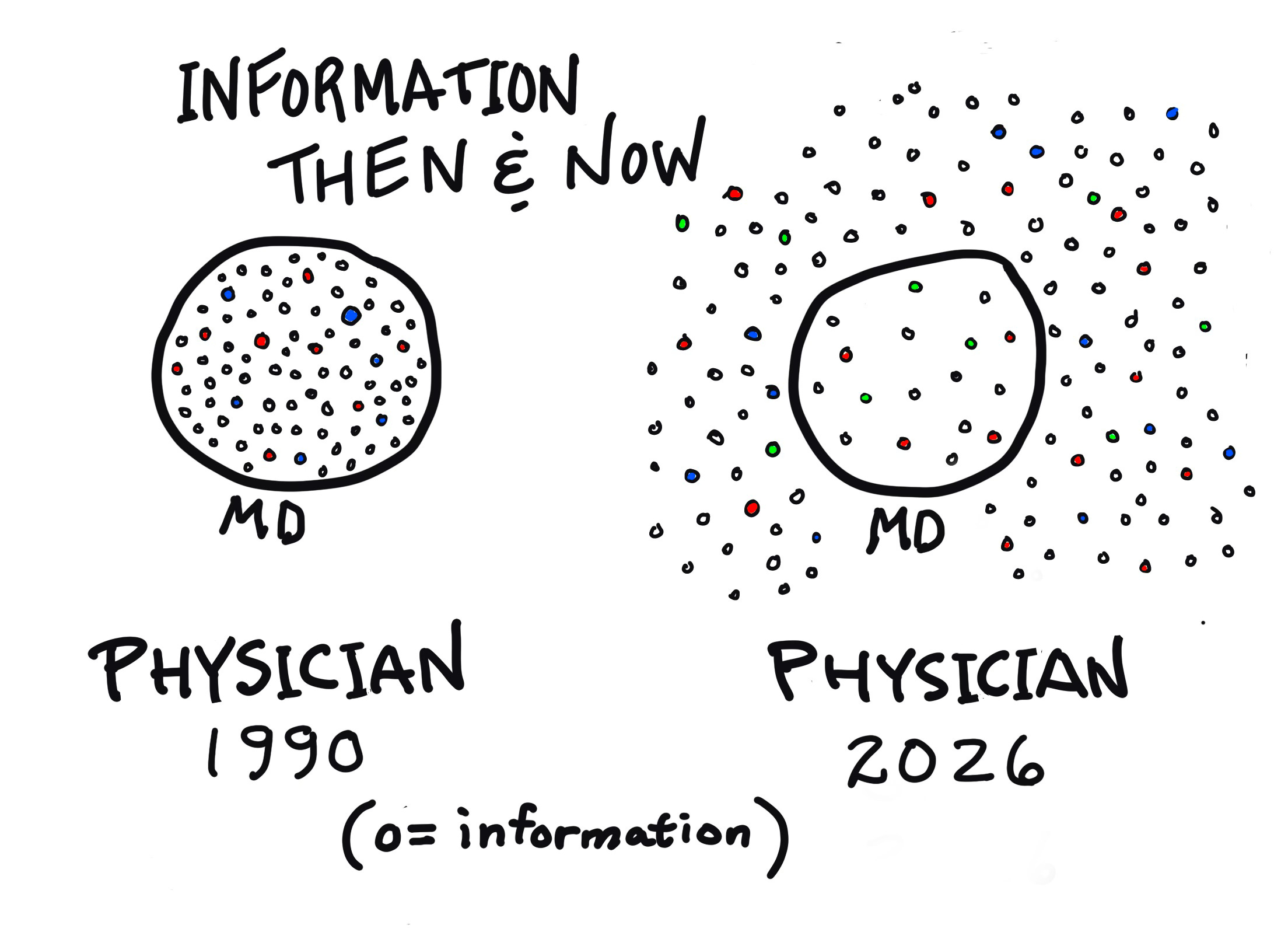
I created the graphic by hand — I hope I was able to capture the point. I’m hoping to do more of these. Let me know what you think!
Not a doc so never heard of mdGPT but glad there's an LLM out there that's more detailed than Chat. Your use is smart. With the knowledge base growing every day, this allows you to quickly keep up with latest findings as well as to check what's in your memory. We all forget. It will be interesting to see where this leads the profession in the future
Our role now is to recognize which questions are appropriate to ask.